病例介绍
患者田某某,男,51 岁,因「一过性言语不清伴左上肢麻木 20 分钟」于 2014 年 11 月 15 日急诊就诊。患者就诊前 2 小时,散步时突然出现言语不清,伴左上肢麻木,上述症状持续约 20 分钟后恢复如常,就诊途中及过程中上述症状无反复。急诊头 CT 提示腔隙性脑梗塞。患者病来无发热、无意识不清、无抽搐等。
既往史:约两周前类似表现一次,持续约 20 分钟后好转。2006 年 7 月曾患蛛网膜下腔出血,于外院行 DSA 检查未见动脉瘤。1999、2006、2009 年曾患「脑梗塞」,遗留左侧肢体活动略欠灵活。高血压病 30 年,血压最高达 220/160 mmHg,平素口服「苯磺酸氨氯地平」「富马酸比索洛尔」,平素血压水平不详。糖尿病 1 年,未系统治疗。
个人史:否认吸烟史。偶尔少量饮酒。否认阳性家族病史。
体格查体:T36.5℃,P 82 次/分,R18 次/分,BP 155/90 mmHg,心肺腹查体未见明显异常。神经系统专科查体:神志清楚,言语流利,问答合理,查体合作。未及注意力,记忆,认知,定时定向力等障碍。颅神经查体未见异常。右侧肢体肌力 5 级,左侧肢体肌力 5 级-,四肢肌张力正常,四肢腱反射对称存在(++)。周身未见肌萎缩及肌束颤动。周身未见深浅感觉障碍。双侧指鼻实验及跟膝胫实验稳准,双侧轮替协调,Romberg 征(-)。双 Babinski 征(-)。脑膜刺激征(-)。
辅助检查
实验室检查:空腹血糖:6.81 mmol/l。血钾:3.21 mmol/l。余未见确切异常。
影像学检查(见图 1),心电图、心脏彩色超声,消化、泌尿超声,经颅多普勒超声均正常。脑电图(-)
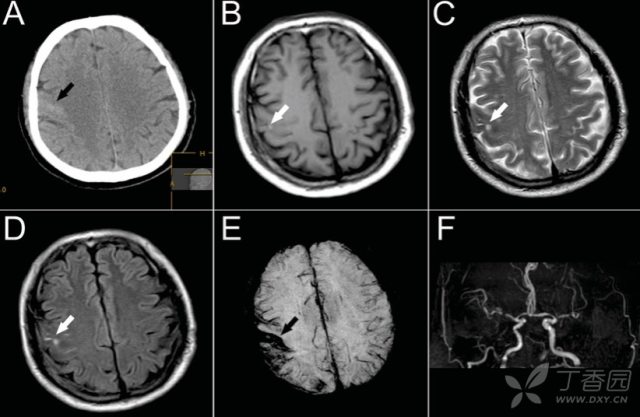
图 1 患者的影像学表现。A:非增强头 CT(2014-11-15)示右侧中央前沟内稍高密度影(黑色箭头)。B~D:颅脑 MRI(2014-11-17):右侧中央前沟内见散在条状 T1 高信号 T2 低信号,部分病灶于 FLAIR 序列呈高信号(白色箭头)。E:SWI 示右侧额顶叶脑沟内磁敏感信号,以中央前沟为甚(黑色箭头)。颅脑 MRA(2014-11-17):双侧颈内动脉岩段、右侧颈内动脉虹吸段、双侧大脑中动脉水平段及右侧大脑前动脉起始段血管狭窄、信号减低。基底动脉及双侧大脑后动脉未见确切显示。
诊断:
1.凸面蛛网膜下腔出血
2.多发脑血管狭窄(双侧颈内动脉狭窄 双侧大脑中动脉狭窄 右侧大脑前动脉狭窄双侧椎动脉 基底动脉、双侧大脑后动脉闭塞)
3.脑梗塞后遗症
4.高血压病 3 级(极高危)
5.2 型糖尿病
6.低钾血症(已纠正)
治疗及随访:予活化脑细胞等治疗,患者住院治疗 10 天后复查头 CT 示右侧中央前沟内高密度消失。患者无不良主诉,嘱其三个月后复查头 MRI。
讨论:
非外伤性凸面蛛网膜下腔出血 (convexal subarachnoid hemorrhage, cSAH) 是蛛网膜下腔出血的一种非典型性表现,该病的出血仅局限于脑顶部的脑沟内,而不涉及相邻脑实质或同侧脑裂,脑池或脑室。因此,凸面蛛网膜下腔出血又被称为皮层蛛网膜下腔出血 (cortical SAH) 或脑沟蛛网膜下腔出血 (sulcal SAH)。
cSAH 的起病形式多样:
根据 Kumar S 等包含 29 名 cSAH 患者的一项回顾性研究,62% 的患者以头痛起病。然而大部分的>60 岁的患者(54%)却以短暂性局灶性神经功能缺损 (Transient focal neurological episodes, TFNE) 起病。
同时 69% 的>60 岁的患者影像学显示脑淀粉样血管病 (cerebral amyloid angiopathy, CAA) 表现,如白质疏松和/或微出血/皮层表浅铁质沉积。
在另一项包括了 24 名患者的观察性研究中,作者也证实了 60 岁以上的患者约有 45% 以 TIA 样表现起病。
cSAH 的可能病因还包括:可逆性后部白质脑病综合征,脑静脉(窦)血栓形成,高血压性小血管病,血小板减少性紫癜,海绵状血管瘤,颅内血管炎,脑脓肿,应用抗凝药物等。
关于本病例 cSAH 的可能原发病因,我们做了以下分析:
首先,结合患者起病特点和实验室检查,头 MRI、SWI、MRA 和 MRV 图像,可以排除动静脉畸形、脑血管烟雾病、主动脉壁夹层形成、血管炎、颅内肿瘤和脑脓肿。
其次,我们排除了 CAA 的诊断。虽然与孤立皮层静脉血栓形成(isolated cortical venous thrombosis,iCVT)鉴别诊断比较困难,但患者无脱水、用药、发热等血液高凝的危险因素,无头痛、恶心呕吐及抽搐等常见症状。同时,反复检验血浆 D-二聚体未见异常。
此外,SWI 影像上脑沟内静脉的信号是规则光滑和均匀一致的,如是 iCVT 则常伴相邻静脉引流区内的血肿;而脑沟内的出血却是形状不规则,边界粗糙的,同时出血信号是非均匀一致的。并且由于血液充满脑沟,异常信号常呈三角形形态(如图 1 所示)。
该患 MRI、MRV 图像未显示静脉内血栓。反复查头 CT 右侧顶叶脑沟内由高密度最终转为等密度信号,更能证明该信号为出血而非静脉血栓。
我们注意到:以 TFNE 样起病的 cSAH 应注意与 CAA 相鉴别:
根据 Charidimou A 等 2012 年发表的一项囊括 172 名 CAA 患者的多中心队列研究,14.5% 的 CAA 患者以 TFNE 起病。
同时,在 CAA 患者最常见的神经影像表现中,54% 的患者表现为凸面蛛网膜下腔出血/皮层表浅铁质沉积。
比较没有 TFNE 的患者,以 TFNE 起病的 CAA 患者更容易发生凸面蛛网膜下腔出血/皮层表浅铁质沉积。
此后的多项研究和病例报道等均证实了 TFNE 与 CAA 的相关性 ,以及 cSAH 与 CAA 疾病的重叠。
磁共振影像对于鉴别缺血源性的 TIA 与出血性的 cSAH 甚至 CAA 至关重要:
大约有 1/3 临床确诊的 TIA 患者表现为 DWI (Diffusion-weighted imaging) 弥散受限信号。由于现代影像学的发展,TIA 的概念正在逐步从强调临床症状的持续时间演变为强调组织学上的细胞死亡。事实上,美国卒中协会已经推荐了基于影像学的尤其是 DWI 序列的,强调脑组织坏死的新的 TIA 概念。
另一方面,临床常用 T2 梯度回声序列或磁敏感序列 (susceptibility-weighted imaging, SWI) 发现脑内亚急性,慢性或微出血。近年来的一些证据表明后者可能比前者更敏。
在临床工作中,以缺血性血管病为病因的 TFNE 我们诊断为 TIA,同时缺血性脑血管病包括了脑梗死,TIA 和静脉血栓形成等。另一方面,cSAH 既可以继发于脑静脉窦血栓形成或孤立皮层静脉血栓形成 (isolated cortical venous thrombosis, iCVT),同时在神经影像上,iCVT 又与 cSAH 相似。另外,正如前文谈到的那样,与非 TFNE 起病的患者相比,以 TFNE 起病的 CAA 患者更容易发生凸面蛛网膜下腔出血/皮层表浅铁质沉积。
综上所述,因为众多疾病谱的相互覆盖(见图 2),在诊断以往被我们所熟悉的「TIA」时,必须结合患者病史、症状体征及辅助检查综合判断,防止盲目下结论影响治疗及预后。
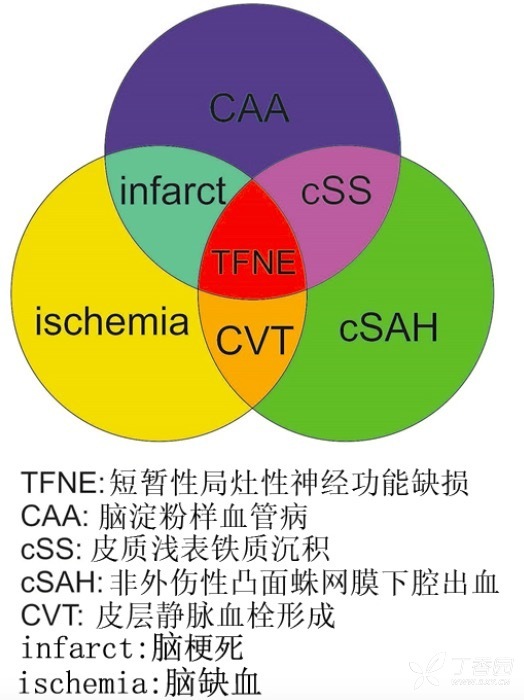
图 2 以短暂性局灶性神经功能缺损为起病临床表现的疾病谱
本文作者:刘培慧 隋轶 徐冰 孙晓红,本文病例来自于沈阳市第一人民医院,
参考文献:
1. Kumar, S., et al., Atraumatic convexal subarachnoid hemorrhage: clinical presentation, imaging patterns, and etiologies. Neurology, 2010. 74(11): p. 893-9.
2. Beitzke, M., et al., Clinical presentation, etiology, and long-term prognosis in patients with nontraumatic convexal subarachnoid hemorrhage. Stroke, 2011. 42(11): p. 3055-60.
3. Ciccone, A., et al., Subarachnoid haemorrhage treated with anticoagulants. Lancet, 2000. 356(9244): p. 1818.
4. Shah, A.K., Non-aneurysmal primary subarachnoid hemorrhage in pregnancy-induced hypertension and eclampsia. Neurology, 2003. 61(1): p. 117-20.
5. van Gijn, J. and G.J. Rinkel, Subarachnoid haemorrhage: diagnosis, causes and management. Brain, 2001. 124(Pt 2): p. 249-78.
6. Spitzer, C., et al., Non-traumatic cortical subarachnoid haemorrhage: diagnostic work-up and aetiological background. Neuroradiology, 2005. 47(7): p. 525-31.
7. Geraldes, R., et al., Nontraumatic convexity subarachnoid hemorrhage: different etiologies and outcomes. J Stroke Cerebrovasc Dis, 2014. 23(1): p. e23-30.
8. Charidimou, A., et al., Spectrum of transient focal neurological episodes in cerebral amyloid angiopathy: multicentre magnetic resonance imaging cohort study and meta-analysis. Stroke, 2012. 43(9): p. 2324-30.
9. Charidimou, A., J.C. Baron, and D.J. Werring, Transient focal neurological episodes, cerebral amyloid angiopathy, and intracerebral hemorrhage risk: looking beyond TIAs. Int J Stroke, 2013. 8(2): p. 105-8.
10. Charidimou, A., et al., Cortical superficial siderosis and intracerebral hemorrhage risk in cerebral amyloid angiopathy. Neurology, 2013. 81(19): p. 1666-73.
11. Apoil, M., et al., Focal cortical subarachnoid hemorrhage revealed by recurrent paresthesias: a clinico-radiological syndrome strongly associated with cerebral amyloid angiopathy. Cerebrovasc Dis, 2013. 36(2): p. 139-44.
12. Linn, J., et al., Prevalence of superficial siderosis in patients with cerebral amyloid angiopathy. Neurology, 2010. 74(17): p. 1346-50.
13. Coates, R., et al., Cerebral amyloid angiopathy: amyloid spells and cortical superficial siderosis. Pract Neurol, 2014.
14. Brazzelli, M., et al., Diffusion-weighted imaging and diagnosis of transient ischemic attack. Ann Neurol, 2014. 75(1): p. 67-76.
15. Albers, G.W., et al., Transient ischemic attack--proposal for a new definition. N Engl J Med, 2002. 347(21): p. 1713-6.
16. Easton, J.D., et al., Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke, 2009. 40(6): p. 2276-93.
17. Sacco, R.L., et al., An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 2013. 44(7): p. 2064-89.
18. Tong, K.A., et al., Hemorrhagic shearing lesions in children and adolescents with posttraumatic diffuse axonal injury: improved detection and initial results. Radiology, 2003. 227(2): p. 332-9.
19. Haacke, E.M., et al., Imaging cerebral amyloid angiopathy with susceptibility-weighted imaging. AJNR Am J Neuroradiol, 2007. 28(2): p. 316-7.
20. Cheng, A.L., et al., Susceptibility-weighted imaging is more reliable than T2*-weighted gradient-recalled echo MRI for detecting microbleeds. Stroke, 2013. 44(10): p. 2782-6.
21. Oppenheim, C., et al., Subarachnoid hemorrhage as the initial presentation of dural sinus thrombosis. AJNR Am J Neuroradiol, 2005. 26(3): p. 614-7.
22. Chang, R. and D.P. Friedman, Isolated cortical venous thrombosis presenting as subarachnoid hemorrhage: a report of three cases. AJNR Am J Neuroradiol, 2004. 25(10): p. 1676-9.
23. Wu, Z., et al., Evaluation of traumatic subarachnoid hemorrhage using susceptibility-weighted imaging. AJNR Am J Neuroradiol, 2010. 31(7): p. 1302-10.
